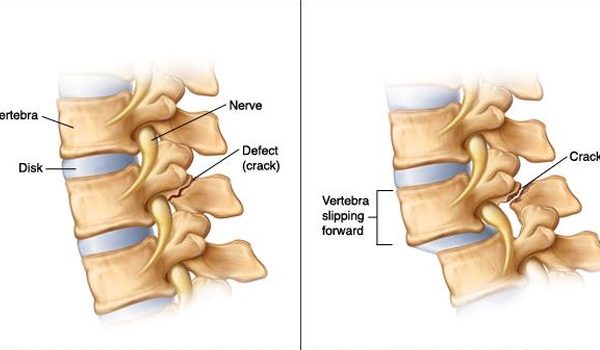
Spondylolysis is a spinal condition that results from a defect in a part of the lumbar vertebra called the pars interarticularis, the thinnest and weakest part of the vertebra. The cause of the defect is not known but is thought to be a combination of repetitive trauma and a genetic weakness that makes the patient susceptible to spondylolysis. Spondylolysis weakens the bones causing dislocation of the vertebrae called Spondylolisthesis.
Spondylolysis is present in up to 6% of the population and is a common cause of low back pain in children and young athletes who are particularly at risk for weakness in the spine while the spine is still growing. Participate in sports like gymnastics, weightlifting, baseball, soccer and football. Boys are more frequently affected than girls.
Spondylolisthesis is the dislocation or slippage between two vertebrae in the lower spine. It may occur as a consequence of congenital defects and/or trauma. Back and leg pain are common, yet many of those affected have no symptoms.
Symptoms
Spondylolysis Symptoms: Spondylolysis is often asymptomatic but can lead to low back pain and swelling particularly during teen growth spurts. The pain may radiate to the buttocks and back of the thighs and worsen with activity. If not treated promptly it can result in spondylolisthesis.
Spondylolisthesis Symptoms: Severe pain, tight hamstrings, stiff back, and difficulty walking and standing. It can cause compression of a nerve root and produce symptoms such as tingling, numbness, and leg weakness.
Diagnosis of Spondylolysis and Spondylolisthesis
Dr. Shufflebarger will review your child’s medical history, general health and symptoms, and discuss the sports in which the child is involved. A physical exam will identify areas of tenderness, range of motion restrictions, muscle spasms and muscle weakness.
Your child’s posture and gait will be evaluated to identify tight hamstrings and awkward or stiff legged gait; and the ability to bend backward and forward. Pain while bending suggests a fracture. To identify a fracture and slippage, X-rays, Bone scans and CT scans will be ordered. An MRI may be ordered to identify a possible nerve root injury, where the slipped vertebra is pressing on a nerve root. It can also identify injury to the vertebra before it can be seen on an x-ray.
Spondylolisthesis is graded low or high grade based on the amount of slippage. High grade means that more than 50% of the fractured vertebra has slipped forward on the vertebrae below it. A high-grade slippage causes significant pain and likely nerve injury thus requiring surgery to relieve symptoms and prevent nerve damage.
Treatment
The goal of treatment is to reduce pain, allow the damage to heal and the patient to return to sports. Most patients with these conditions will improve with conservative treatment. Treating early can restore function, provide pain relief, and help to avoid chronic back pain and loss of flexibility. Current studies report that conservative treatment for Grade 1 spondylolisthesis can be successful. However, if a patient with progressive Spondylolisthesis fails to improve with conservative treatment for six weeks, surgery may be indicated. Dr. Shufflebarger authored the chapter on “Surgical Treatment of Spondylolisthesis” in the prestigious Text book of Spinal Surgery.”
Conservative Treatment
Cessation of sports activity for 3-6 months only starting back when pain free
- Rest
- Core strengthening
- Flexibility training
- Physical therapy
- Anti-inflammatory medication
- Bracing – studies report that conservative treatment can succeed without the use of a brace.
The addition of low-intensity pulsed ultrasound for early spondylolysis in young athletes and for patients with progressive spondylolysis aids in bone healing.
Surgery
When the child has persistent back pain (for more than six months) or severe slippage of the vertebrae surgery is indicated to relieve symptoms and restore mobility. Spinal fusion of L5 and the sacrum is the most common surgical procedure. If the slippage is compressing a nerve root, an additional procedure will relieve pressure on the nerve before fusion. Return to play for elite athletes following surgery varies from 6 to 12 months for non-collision sports.
Dr. Harry L. Shufflebarger is a board-certified pediatric orthopedic surgeon and a nationally and internationally recognized expert in the care of all pediatric spine disorders, including scoliosis. In addition to his many accomplishments in research and innovation in pediatric spine conditions, he is a kind and compassionate doctor who is sought out by parents the world over.