A spine fracture is a serious injury. Young men are the most frequent victims of a fracture of the spine caused by high-energy trauma from falls and traffic accidents. Neurological injury occurs in 16 -25% high-energy traumas. Most spine fractures occur in the mid or low back or at the juncture between the two and constitute a substantial risk of spinal cord injury and paralysis.
Many traumatic spine fractures can be treated with conservative measure including 4-12 weeks of immobilization and bracing. However, major fractures that cause instability, and those that involve the spinal cord and/or nerve roots will require prompt treatment to reduce the risk of further injury and to minimize long-term disability. Fractures are categorized by the pattern of injury. There are three categories of spine fractures:
1. Flexion – Fracture Pattern
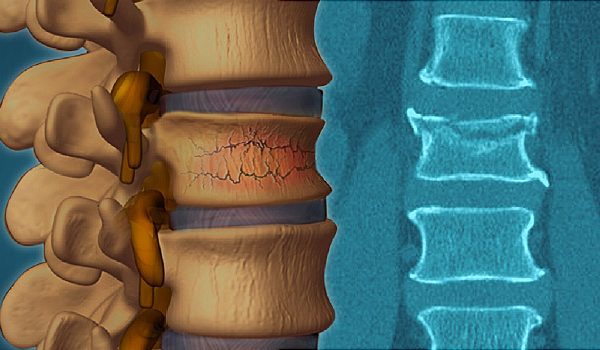
Compression fractures
Compression fractures are the most common type. In a compression fracture the injury causes the vertebrae to collapse causing acute pain, usually severe. Compression fractures involve a breakage of the front of a vertebra but not the back. These fractures tend to be stable meaning the bones will not move out of place. Most flexion fractures can be treated without surgery when the fracture is stable. Vertebroplasty, injection of a cement material into the vertebral body, may shorten the recuperation.
Burst Fractures
When the trauma is in the right direction and forceful enough, it can burst the bone sending bone fragments in all directions , including into the spinal column. Burst fractures are frequently unstable and increase the risk of long-term neurological damage. Unstable burst fractures are a medical emergency. They are treated with surgical decompression of the spine and stabilization of the fracture.
2. Extension – Fracture Pattern
Flexion-Distraction Fractures
Flexion-Distraction Fractures are often called “Chance Fractures” or “Seat-belt fractures”. They occur when traumatic forces pull the posterior portion of the vertebrae apart. This is often caused by a head – on collision where the chest is thrown forward, and the lower body is held stable by a seat belt. The trauma fractures the bone and may tear the ligaments. Severe back pain is the main symptom. This pattern may damage internal organs and be associated with other injuries.
If there is no damage to the ligaments, vertebral discs or spinal cord, extension fractures can be treated nonsurgical with bracing or casting for 3 months. . Surgery may be necessary with significant kyphotic deformity, ligamentous injury, or neurologic signs or symptoms.
Rotation Fracture Pattern:
The most common rotation pattern is found in fracture – dislocation where the vertebra is displaced or dislocated and compresses the spinal cord. This is a very unstable injury that causes severe pain and when the spinal cord is involved, may produce numbness, tingling, weakness and even bowel and bladder dysfunction. This is a medical emergency. These fractures require stabilization with posterior spinal fusion and vertebrae realignment.
Symptoms of a spinal fracture
Symptoms vary depending on the location and type of fracture. The first symptom is pain and worsening of pain with movement. However, when the spinal cord is involved symptoms include numbness, tingling, weakness, bowel and bladder dysfunction, and paralysis.
Diagnosis
Emergency stabilization at the scene of an accident is necessary before transfer to the ER. Arriving at the ER, the trauma specialist will assess the extent of injuries, including breathing ability. The patient will be examined head to toe. X-rays will reveal the type and severity of the fracture. A CT scan will provide 3-D views to reveal all bone damage, and diagnose soft tissue injuries, and bleeding. An MRI with contrast will provide a clear view of damage to ligaments discs and the spinal. The trauma doctor will conduct a neurological exam.
Treatment
Initially treatment will the focus on pain management and stabilization to prevent additional injuries. When there are other injuries, they will also be treated. When the fracture only affects the vertebrae, and the spine is stable , nonsurgical treatment with a brace or cast will be sufficient. Depending on the fracture pattern and stability, bracing and possibly surgery will be needed. 8-12 weeks of bracing may be required. Instrumentation and fusion are surgical procedures to treat unstable fractures. Minimally invasive surgical procedures will be used to treat compression fractures